
Since the novel coronavirus (SARS-CoV-II) was identified in Wuhan, China, in December 2019, it has spread rapidly, initially all over China and then throughout the entire world, reaching Palestine on March 5, 2020, when the first imported cases of COVID-19 were identified in Bethlehem. The Palestinian government’s response was swift and effective: H.E. President Mahmoud Abbas declared a state of emergency, and Prime Minister Dr. Mohammed Shtayyeh took responsibility for implementing the various measures necessary in this situation.
Prime Minister Dr. Shtayyeh established the inter-ministerial and multilateral High-Level National Emergency Committee, supported by national emergency subcommittees at the district level. The governmental approach in battling COVID-19 was built on the principles of preparation, containment, and communication. The Palestinian government issued its National COVID-19 Response Plan in March 2020, outlining its response strategy and actions, identifying critical support needs, and proposing an aid coordination approach.
The Ministry of Health (MoH) was attentive to the upcoming outbreak once it started to spread outside China in mid-January 2020, and devoted keen internal efforts to prepare for the pandemic on various sides. MoH early action included conducting health education and staff training regarding the virus and related infection-control measures followed by early-detection measures on borders.
The Palestinian Ministry of Health responded quickly and effectively to the outbreak of COVID-19, mobilizing all its efforts and resources to contain the spread of the virus.
The COVID-19 National Health Readiness Plan, developed by the MoH in coordination with various national stakeholders and continuously reviewed and updated according to the situation, aimed to scale up readiness capacities to face the pandemic while also ensuring the continuity of essential health services and the sustainability of the health system. The MoH approach was focused on containment, response, and resilience.
Epidemiological phases and crisis management
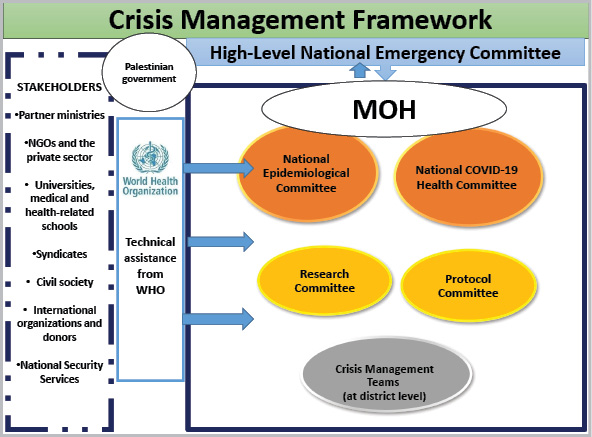
The management of the various health aspects of the crisis in Palestine is led by the MoH and technically supported by the World Health Organization (WHO). The MoH coordinates and cooperates with all sectoral stakeholders, including nongovernmental and private health sector institutions, civil society organizations, academic and research partners, partner ministries and security services, UN agencies, and the international community. Upon identifying the first cases in March, the MoH took the immediate decision to establish the National COVID-19 Health Committee and the National Epidemiological Committee to take on the responsibility for the continuous follow-up of the epidemiological situation and give its recommendations to the High-Level National Emergency Committee. Both the National COVID-19 Health Committee and the National Epidemiological Committee include representatives of various relevant stakeholders and receive technical support from the WHO (Figure A). On the level of governorates, health teams were part of the various crisis management teams that operate at the district level, headed by the respective governors.
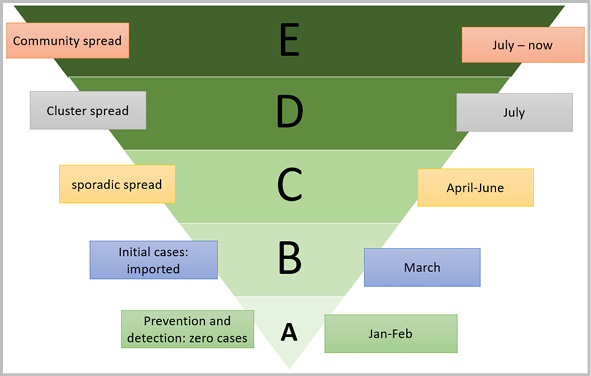
The crisis-management and response-planning process was built on predictable epidemiological phases or probable spread stages. Accordingly, the MoH started to develop its plans and prepare its health facilities according to expected probable spread of infected cases and epidemiological status (Figure B).
The Palestinian government has taken an evidence-based, proactive approach of containment and suppression in the early stages, supported by a national health awareness campaign to encourage our citizens to protect themselves and follow governmental guidance of movement restrictions and social distancing. This approach succeeded in limiting community transmission during the first three months (April through June 2020). Government actions aim to protect its citizens and prevent the uncontrollable spread of the virus and the resulting health system challenges that occurred in other countries. At the same time, substantial efforts were made to ensure adequate diagnostics and treatment services, on the one hand, and to prepare for a potential surge of cases on the other.
COVID diagnostic services
One of the most preliminary preparatory actions that the MoH took was the capacity building of the Central Public Health Laboratory concerning the diagnosis of COVID-19 through staff training and the provision of laboratory diagnostic materials for the testing and detecting of the virus. The Central Public Health Laboratory in Ramallah has been able to conduct COVID-19 diagnostic tests since February 6, 2020.
As the incidence of COVID-19 cases increased in several governorates, the number of contacts and potential or suspected cases who required testing increased accordingly, and the urgent need arose to expand our diagnostic capacity. Thus, in partnership with several universities and nongovernmental hospitals, the MoH established PCR labs in governorates outside Ramallah and Al-Bireh. We now run seven active PCR labs in various governorates and have succeeded in raising our testing capacity from 300 tests per day in February to 7,000 tests per day in November.
Quarantine and isolation policies
At the beginning of the pandemic outbreak in Palestine, in early March, the government adopted facility-based quarantining. It started to establish quarantine centers for suspected cases and individuals who came from outside the country through the border crossings at Jericho and Rafah. The Palestinian Academy for Security Sciences in Jericho was the first established quarantine center in the West Bank, followed by special centers established in each governorate in cooperation with various community organizations. The MoH adopted WHO instructions in this regard, requiring a 14-day quarantine period for contacts and suspected cases; later on, we adopted the home-isolation policy for mild and asymptomatic cases. Moderate and severe cases are admitted to specified treatment centers.
COVID-19 epidemiological surveillance systems
The MoH took steps to guarantee the early detection of cases as much as possible. In addition to screening services on borders and entry points, and establishing triage centers for any suspected case in all health facilities and hospitals, the MoH involved contact tracing and following up suspected cases, drawing up epidemiological contact trees through data collected from infected cases. Also, the MoH in cooperation with the National Security Services used geographical data to track home-quarantined cases.
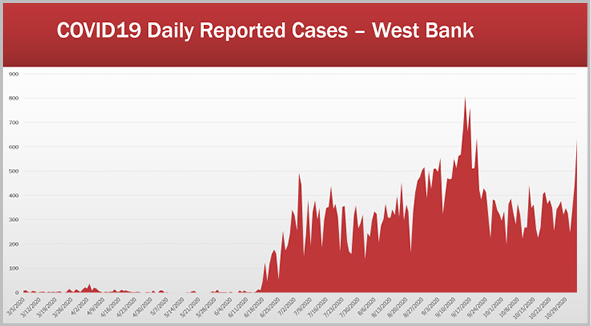
Even though COVID-19 has spread widely in the Palestinian community since late June (Figure C), the recovery rate is considered very good, and the fatality rate in Palestine is relatively low compared to other countries in the region.
In cooperation with the Palestinian National Institute of Public Health, the MoH established the Electronic COVID-19 Epidemiological Surveillance System accompanied by a publicly accessible website that presents regularly updated data on the situation in Palestine, including the distribution of cases by age and location and health maps.*1 Furthermore, the MoH developed two mobile applications for the community. The online portal lets people obtain their test results online, which made it much easier to follow up on suspected cases,*2 and the newly developed application Amankom is intended to enable the tracing of potential COVID contacts via mobile phones.*3

Hospital preparedness
The MoH developed a special emergency COVID response plan for Palestinian hospitals that aimed to upgrade the hospital sector’s preparedness for COVID-19 and identify hospitals assigned for COVID treatment. Seven such hospitals have been established and equipped, including Hugo Chavez Hospital in Turmus Ayya, Dura Hospital, Security Academy in Jericho, Addiction Rehabilitation Center in Bethlehem, Military Services Hospital in Nablus, Azzoun Health Center, and Qashda Treatment Center. Several other general hospitals have some dedicated beds for COVID patients. Moreover, the MoH has made tremendous efforts to increase the number of beds, ICU beds, and ventilators allocated for COVID-19 patients, and we have succeeded in making available at this time a total of 603 beds, 189 ICU beds, and 152 ventilators.
Technical instructions and protocols
As the WHO is considered the main technical assistant worldwide in battling the novel coronavirus pandemic, the MoH and the National Epidemiological Committee have followed up continuously on WHO recommendations and technical updates and have issued their technical instructions for health teams and the general public accordingly. Several technical health protocols were developed, most importantly the Palestinian National COVID-19 Management Protocol, authored by a specially assigned national medical committee composed of medical experts and specialized doctors. Another important protocol issued by the MoH is the National Protocol for Living with COVID (And Life Continues [in Arabic]) that includes public safety guidelines and measures to be followed by citizens to protect themselves from becoming infected.
Health workforce
The COVID-19 pandemic has profoundly impacted the health care workforce. As cases surged across the country, the workload has increased tremendously, especially for staff working on the front line, such as diagnostic lab technicians, preventive medicine teams, those in treatment centers, and more. On the one hand, there has been the urgent need to build their capacities and enable them to face this new global pandemic, on the other, staff must protect themselves from the high risk of infection.
The MoH thus took immediate action to provide adequate PPE for its health care workers and train its staff. Special training materials and training curricula were developed, targeting the various health workforce specialty categories. Recently, a national training program was established with the support of NGOs, targeting health care workers in both the public and private health sectors. At the same time, the government has started to hire additional staff through temporary contracts supported by the World Bank and UNDP.

Challenges
The Palestinian health care system has been suffering tremendous challenges due to the decades-long military and economic occupation. The COVID-19 pandemic coincided with the Israeli withholding of Palestinian tax revenues and annexation plans that further worsened the economic situation and deepened the ongoing financial crisis.
Thus, the State of Palestine is doubly handicapped in its fight to contain the COVID-19 pandemic. We lack the necessary sovereignty (such as control over borders, etc.) and national resources (medical, financial, etc.) to cope with a significant outbreak, particularly as our population has many high-risk characteristics (crowded cities and refugee camps, poverty, food insecurity, noncommunicable diseases, etc.).
The Palestinian humanitarian and health conditions were already fragile, even before COVID. Palestinians who live in overcrowded areas and miserable camps find it difficult to practice physical distancing; prisoners confined in Israeli jails are at a high risk of infection and deprived of their right to health; and Palestinian patients have been largely forbidden to seek treatment outside the country, as all borders are officially closed. Israeli occupation policies in East Jerusalem and the ongoing siege of the Gaza Strip have hindered our capacity to ensure the necessary services for large segments of COVID-19 patients. Palestinian workers inside Israel have posed a main challenge, especially those who travel daily to and from Israel without any protective measures and are considered a high risk for the wide spread of COVID-19 from Israel to Palestine, as for many months, the situation in Israel was much worse than in Palestine.
The health system is overstretched, with high rates of noncommunicable diseases, shortages in terms of a specialized health care workforce on both the governmental and private national levels, with shortages in hospital beds and gaps in specialized care services. Community beliefs and resistance to the reality of the pandemic have further hindered our efforts.
*1 COVID 19 Epidemiological Surveillance System, MoH, published on MoH website, available at http://site.moh.ps/index/covid19/LanguageVersion/0/Language/ar.
*2 Ibid.
*3 The MoH COVID-19 portal to view test results is available at https://result.moh.ps/.
